
The Post-Spike Blind Spot
Why Long COVID, vaccine injury, and nattokinase deserve a more honest conversation


A meaningful share of what is currently labeled “Long COVID” may be better understood as a post-spike syndrome — one that can follow infection, vaccination, or both. The evidence is no longer thin enough to ignore, and the intervention with the strongest mechanistic fit happens to be a fermented legume enzyme that no one can patent.
Overview
The central question raised by my previous investigation is whether a meaningful share of what is currently labeled “Long COVID” may be more accurately understood as a broader post-spike and systemic toxicological syndrome associated with exposure to novel biotechnological interventions, environmental stressors, immune dysregulation, endothelial injury, microclotting phenomena, mitochondrial dysfunction, and latent biological processes that have been narratively framed within a virological paradigm.
Rather than presuming the correctness of prevailing assumptions regarding viral causation, transmissibility models, or pharmaceutical countermeasures, this investigation examines whether the dominant explanatory framework itself may be incomplete, circular, or fundamentally mischaracterized. It asks whether persistent spike-related pathology, inflammatory signaling cascades, endothelial damage, immune perturbation, and what are often described as “viral reactivation” events may instead reflect broader stress-response biology, toxicological injury patterns, exosomal signaling phenomena, or dysregulated adaptive processes that have been interpreted through the lens of institutional virology.
Under this view, the category “Long COVID” may function less as evidence of a singular pathogenic entity and more as an umbrella construct encompassing heterogeneous chronic illness states with overlapping biological signatures and potentially divergent origins — including exposure to synthetic spike-producing technologies, environmental toxicants, chronic inflammatory burden, electromagnetic stressors, metabolic dysfunction, or other unresolved contributors.
The materials reviewed here collectively press three claims:
First, toxic and iatrogenic injuries can mimic infectious syndromes so convincingly that clinicians can miss the true cause.
Second, spike protein itself is biologically active enough to serve as a plausible driver of chronic, multisystem dysfunction, regardless of whether its source is infection or vaccination.
Third, nattokinase — a food-derived enzyme from fermented soybeans with a long history of dietary exposure — deserves serious attention as a candidate intervention because it degrades spike protein in vitro and also carries a substantial literature relating to fibrinolysis and vascular support.
A Broader Framework for Post-Pandemic Illness
My Poisoned, Not Infected series argues that modern medicine too often defaults to a pathogen-only explanation even when toxic exposures, pharmaceutical effects, and the body’s own stress signaling may be producing an illness pattern that looks infectious. That framing is developed across the attached essays:
Poisoned, Not Infected: Why Your Body’s Healing Response Looks Like Disease
Poisoned, Not Infected: Reinterpreting Viral Disease through Chemical Toxicity
Reframing Viral Mechanisms: Exosomes, Toxicity, and the Xenogen Hypothesis
All of these emphasize extracellular vesicles, toxic injury signaling, and the possibility that some disease clusters are being misread through an overly narrow germ-theory lens.
The most compelling part of that broader argument is not its most speculative edge, but its insistence on differential diagnosis. Toxic injury can look infectious, shared exposures can create outbreak-like clustering, and stressed cells can export inflammatory signals through extracellular vesicles that propagate damage without requiring a classic pathogen-centered model for every symptom pattern. Once that possibility is granted, the Long COVID story becomes less settled than public messaging often suggests: persistent post-pandemic illness may include true post-infectious syndromes, post-vaccination syndromes, environmentally amplified inflammatory states, and mixed cases that have been grouped together because the label “Long COVID” is administratively convenient.
Long COVID and Post-Vaccination Syndromes Share a Biological Center of Gravity
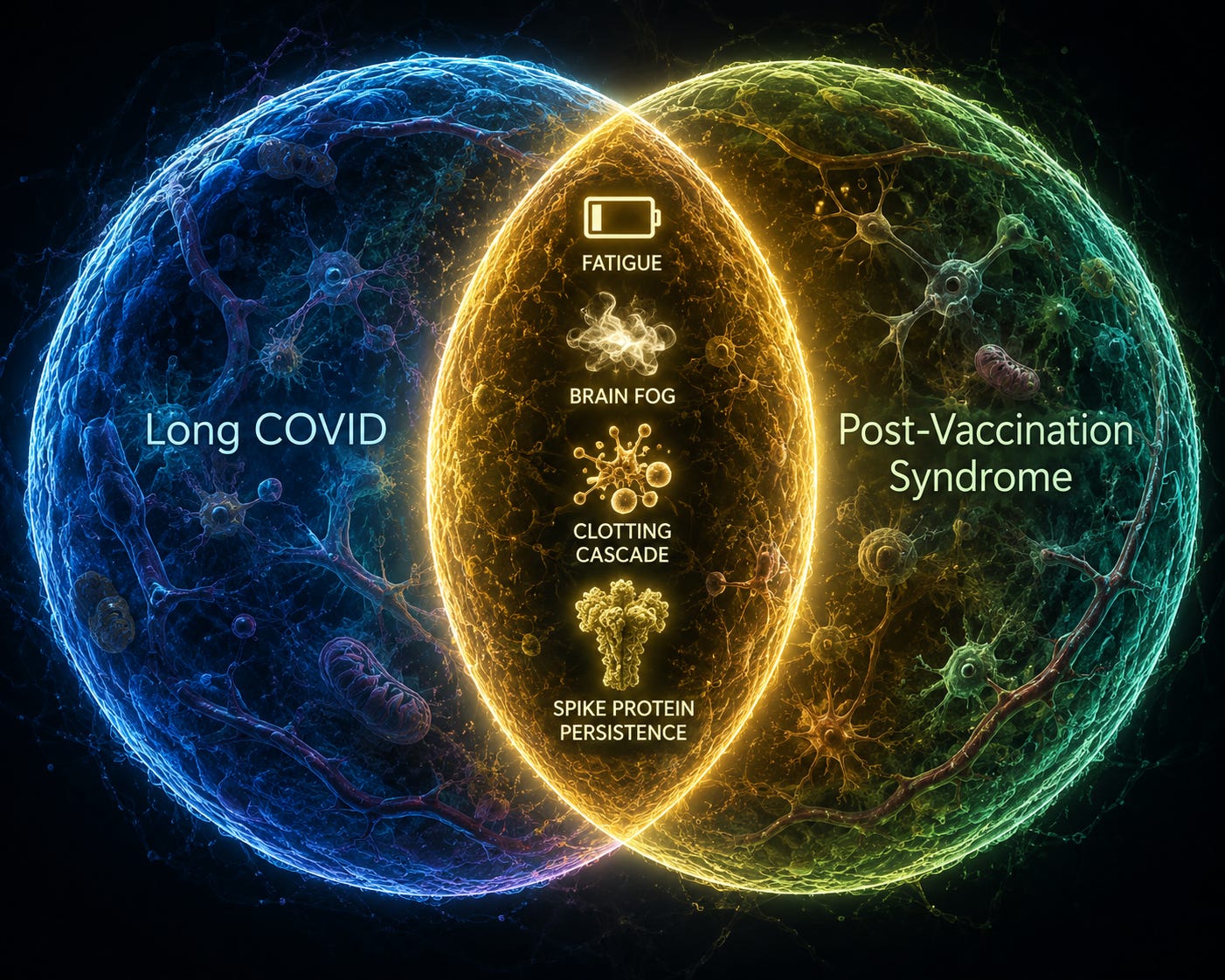
The case for re-examining Long COVID rests heavily on overlap. My previous article Unmasking the Long COVID Cover Story for Vaccine Injury argues that Long COVID and so-called Long Vax or post-vaccination syndrome share a striking cluster of features:
Fatigue
Brain fog
Dysautonomia
Neuropathic symptoms
Exercise intolerance
Endothelial dysfunction
Microclotting
Latent virus reactivation (aka, xenohormetic exosomal activation)
Persistent spike-related findings
That overlap is not, by itself, proof of misdiagnosis, but it is enough to justify studying the two groups side by side rather than preserving a politically comfortable separation.
The retracted IDCases paper on “Post spike syndrome (PSS)” moved directly into this space by describing five patients with chronic symptoms after infection or vaccination and framing them under a single post-spike model. It was a weak case series by conventional standards — small, uncontrolled, and hypothesis-generating at best — but the significance of the paper was conceptual: it treated infection-derived and vaccine-derived spike exposure as potentially convergent causes of chronic illness rather than as distinct silos. That is precisely the move that many institutions remain reluctant to normalize, even though the idea of vaccine-associated adverse effects is already acknowledged in narrower contexts by mainstream regulators and safety agencies.
The broader literature does not support a simple claim that all Long COVID is vaccine injury, and no responsible synthesis should say that. But the evidence does support a narrower and still important claim: chronic post-acute illness after the pandemic likely contains biologically heterogeneous groups, and a model centered on persistent spike burden or spike-triggered pathology is plausible enough to justify much more explicit differentiation between post-infectious and post-vaccination cases.
Why Spike Protein Remains a Plausible Root Cause
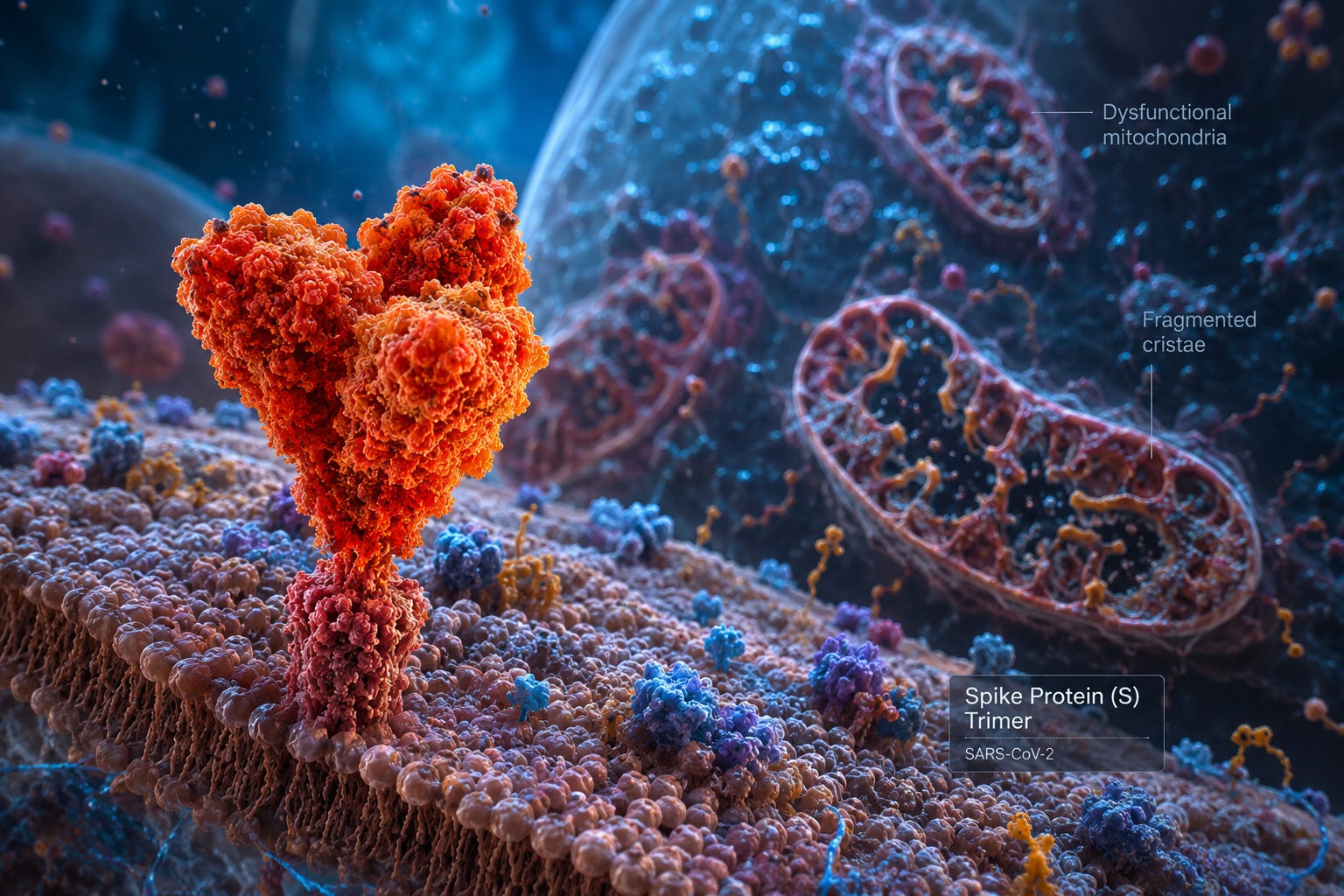
The plausibility of spike protein as a root cause of chronic symptoms does not depend on rhetoric; it depends on whether spike is biologically active, persistent in some people, and capable of driving the kinds of vascular and immune abnormalities seen in Long COVID-like syndromes. The materials reviewed here consistently point in that direction.
A key mechanistic anchor is the 2022 Molecules paper by Tanikawa and colleagues, “Degradative Effect of Nattokinase on Spike Protein of SARS-CoV-2”. In that study:
Nattokinase degraded SARS-CoV-2 spike protein in a dose- and time-dependent manner in transfected cell systems
It reduced spike present on the surface of cells
It did so without reducing cell viability in that model
The authors framed the work as a possible antiviral strategy, but its implications are broader: if spike is a harmful target worth degrading during acute infection, then the same logic naturally extends to post-acute syndromes in which spike or spike fragments may persist and continue to provoke injury.
This is where the attached essays and the PSS case series converge. The essays repeatedly argue that persistent spike, microvascular dysfunction, and immune dysregulation may underlie a substantial share of chronic post-pandemic illness, whether it is attributed to infection or vaccination. The PSS paper tried to operationalize that claim clinically by treating patients whose symptoms arose after one or the other exposure with a protocol that included nattokinase.
The Retraction Story and What It Reveals
My previous essay, When the Retraction of a Spike Protein/Nattokinase Study Itself Becomes the Evidence, interprets the December 2025 retraction of the IDCases PSS paper as a small but revealing example of scientific gatekeeping. The retraction notice stated:
That publication might encourage premature adoption of unvalidated treatments
That there was no empirical evidence supporting a link between the described pathophysiology and vaccines
That the risk of harm outweighed the benefits of continued publication
That notice is striking for two reasons. First, it did not accuse the authors of fabrication, plagiarism, or ethical misconduct; instead, it objected to the potential downstream use of the paper and to the pathophysiological framing itself. Second, the categorical claim that there is “no empirical evidence” linking relevant pathophysiology to vaccines is difficult to square with the broader safety literature, including:
The reanalysis by Fraiman and colleagues in Vaccine reporting excess serious adverse events of special interest in the pivotal mRNA trial data
The public recognition by safety agencies that some inflammatory complications, such as myocarditis and pericarditis, are causally associated with mRNA COVID-19 vaccines
That does not validate the PSS case series as strong evidence. It does, however, reinforce the perception that there is institutional asymmetry: mechanistic biochemistry on spike degradation can remain in the literature, while clinical work that connects spike persistence, post-vaccination injury, and a non-patentable intervention is treated as uniquely dangerous. For advocates of the broader post-spike model, the retraction is not proof of efficacy; it is evidence that some hypotheses are being removed before they are seriously tested.
Why Nattokinase Deserves Serious Attention
Nattokinase is not a novel synthetic pharmaceutical. It is a serine protease produced during the fermentation of soybeans into natto, a traditional Japanese food with a long history of human consumption. That matters because it places nattokinase in a different moral and regulatory category from newly introduced proprietary molecules: the intervention is food-derived, inexpensive, and already well known in the cardiovascular and fibrinolytic literature.
Its appeal in the post-spike context comes from the convergence of several properties:

If persistent spike contributes both to direct inflammatory injury and to pathological fibrin dynamics, then nattokinase is unusually well positioned as a candidate because it is not merely a symptom suppressor; it plausibly addresses both the antigenic target and part of the downstream vascular terrain.
This does not mean nattokinase has already been proven effective for Long COVID or post-vaccination syndrome by randomized controlled trials. It means something narrower and still clinically important: nattokinase is a low-cost, biologically plausible, food-derived compound with a favorable historical exposure profile and a mechanism that maps directly onto one of the strongest available hypotheses for persistent post-pandemic illness.
The Problem of Evidence Standards for Unpatentable Therapies

One reason nattokinase remains on the margins of mainstream treatment discussion is structural rather than scientific. Large randomized trials are expensive, and they are typically financed when a sponsor can own, patent, and profit from the intervention. Nattokinase is not that kind of product. It is a food-derived enzyme sold as a supplement, meaning the economic machinery that funds pharmaceutical-scale validation is much weaker.
This creates a circular evidentiary trap:
Critics can say nattokinase should not be discussed clinically until it has pharmaceutical-grade trial support, while the very features that make it accessible and attractive — its low cost, supplement status, and lack of exclusivity — reduce the likelihood that such trials will ever be funded at scale.
In practice, that means patients and clinicians are left to navigate on the basis of mechanistic evidence, toxicology and safety literature, and lower-tier clinical observations rather than waiting for an ideal evidence hierarchy that may never be built for a non-patentable intervention.
For post-spike syndromes, that issue is especially acute because many patients are sick now, with no approved, uniformly effective treatment pathway. In that context, dismissing nattokinase because it is “only” a food-derived compound or because its evidence base is not yet pharmaceutical in scale is not a neutral scientific posture; it may function as a systematic bias against precisely the kinds of low-cost interventions that are most accessible to patients.
An Advocacy Case for a Post-Spike, Nattokinase-Centered Research Agenda
The most responsible advocacy position is not that nattokinase has solved Long COVID. It is that the post-spike hypothesis is now plausible enough — and the overlap between Long COVID and post-vaccination syndromes substantial enough — that suppressing or marginalizing this line of inquiry is no longer defensible.
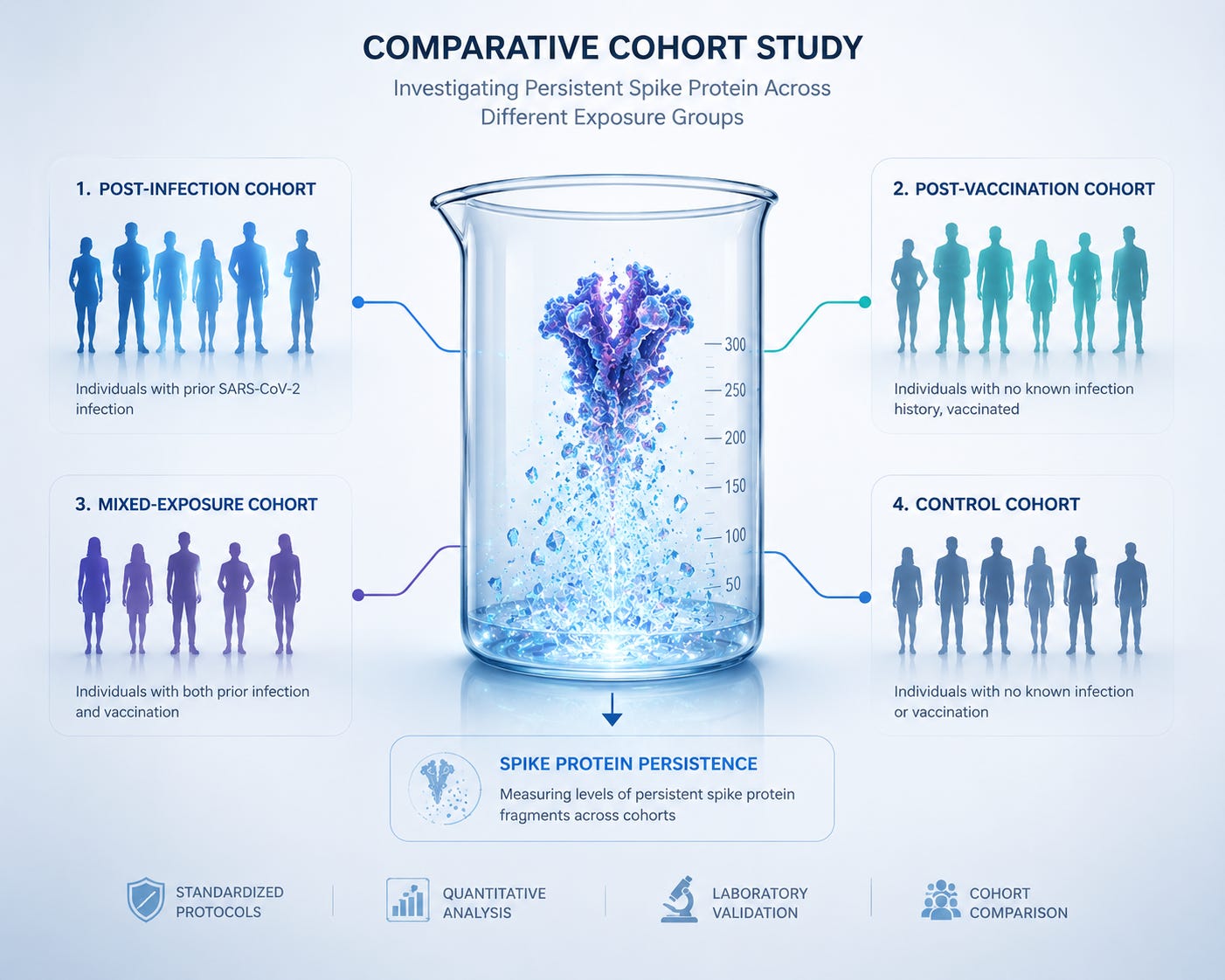
A serious agenda should include several commitments:
Separate cohorts. Distinguish post-infectious, post-vaccination, and mixed-exposure cases instead of treating “Long COVID” as a single undifferentiated bucket.
Measure mechanism, not just symptoms. Track persistent spike, fibrin abnormalities, endothelial markers, and immune dysregulation longitudinally in all groups.
Run formal pilot trials of nattokinase with careful safety monitoring, especially in relation to bleeding risk, anticoagulant use, and baseline cardiovascular status.
Compare spike-targeted protocols with symptom-only management, because a spike-targeted strategy should be judged on whether it changes mechanism-linked outcomes rather than only subjective symptom scores.
Such a program would not require accepting every speculative claim in the broader Poisoned, Not Infected framework. It would simply require acknowledging that spike persistence is a coherent biological target, that post-vaccination injury is real enough to deserve integration into post-acute syndromic research, and that food-derived compounds with direct mechanistic relevance should not be excluded from serious investigation because they are not proprietary drugs.
Conclusion

Taken together, the essays, the nattokinase biochemistry study, the PSS case series, the retraction notice, and the broader vaccine safety literature point toward an uncomfortable but increasingly plausible conclusion: a meaningful portion of chronic post-pandemic illness may be better understood as a post-spike syndrome rather than as a purely post-viral one. That does not erase the reality of Long COVID after infection; it widens the lens to include vaccine-related injury, mixed etiologies, and the possibility that persistent spike protein is a common pathological denominator across categories.
Within that broader view, nattokinase stands out not because it is fashionable, but because it is unusually well matched to the problem:
Food-derived rather than newly synthetic
Inexpensive rather than proprietary
Historically familiar rather than exotic
Mechanistically relevant — it degrades spike protein while also intersecting with fibrinolytic and vascular pathways that may matter in post-spike illness
In a medical culture that too often confuses lack of commercialization with lack of value, nattokinase may be precisely the kind of intervention that deserves more attention, not less.
To learn more about the potential benefits of nattokinase to cardiovascular health, view the most popular article of the year below:
Source Links
Primary research:
Tanikawa et al. (2022). Degradative Effect of Nattokinase on Spike Protein of SARS-CoV-2. Molecules 27(17): 5405. — Full text
Hulscher, Procter, Wynn, McCullough (2023). Clinical Approach to Post-acute Sequelae After COVID-19 Infection and Vaccination. Cureus. — PMC10663976
Fraiman et al. (2022). Serious adverse events of special interest following mRNA COVID-19 vaccination in randomized trials in adults. Vaccine. — DOI:10.1016/j.vaccine.2022.08.036
Yale LISTEN Study / Iwasaki lab updates on post-vaccination syndrome — Yale News, February 2025
Patient and clinical commentary:
We have “post-vaccination syndrome.” We are tired of being used to score anti-vax points. STAT News, June 2025. — statnews.com
Halma & Varon (2025). Breaking the silence: Recognizing post-vaccination syndrome. Heliyon.
Background and framework essays:
Sayer Ji. Unmasking the “Long COVID” Cover Story for Vaccine Injury (Substack)
Sayer Ji. Poisoned, Not Infected: Why Your Body’s Healing Response Looks Like Disease (Substack)
Sayer Ji. Reframing Viral Mechanisms: Exosomes, Toxicity, and the Xenogen Hypothesis (Substack, April 30, 2025)
Sayer Ji. When the Retraction of a Spike Protein/Nattokinase Study Itself Becomes the Evidence (Substack)
Public health context:
CDC. Long COVID in Adults: United States, 2022. NCHS Data Brief No. 480. — cdc.gov
Mayo Clinic. Long COVID: Lasting effects of COVID-19. — mayoclinic.org
I was very glad to read this. I’ve been taking Nattokinase since 2020 after reading about its effectiveness against Covid & long covid. I was fortunate to never get Covid, largely I’m sure due to all the excellent information gleaned from the Disinformation 12 (thank you, Sayer Ji!). Not only did I not get Covid, despite no masking, social distancing, and continuing doing my own in person shopping, I’ve not been sick with anything else either. Lots of supplements, lots of sunshine, lots of exercising and socializing, has kept me healthy at 73! I’ve been able to help my family, close friends and neighbors stay well by passing along the info I’ve learned. Thank you for doing this research and sharing it…I will be passing along this post as well!
I had neither covid 'shot' nor covid; however last year a smart meter was activated in my home (after I had asked to sign a waiver to refuse). My symptoms were identical to the reported 'long covid'. The non-native emfs are 'square waveforms with "spikes"'. How convenient to use a non-specific PCR tests??? When I had asked medical doctors if the 'spikes' from the non-native waveforms may be activating our body's spike proteins, the response is that is 'an interesting question'. According to an electrical engineer, 'it is possible' these waveforms could be activating our own spike proteins. We are bombarded daily with these emfs--computers, wifi, cell towers, 5G, etc. I believe there are factors other than vaccines, or viruses that activate our spike proteins, and one of those may be the non-native emf frequencies? We seem blinded by this possibility because we cannot see. [Gratefully, I was able to get the smart meter removed from my home].